NF1 is a very unpredictable disorder. It varies widely in severity from one person to the next, even between two people in the same family. Some people with NF1 go through life with only a few café-au-lait spots or neurofibromas, while others may have major cosmetic or medical problems due to NF1.
Such uncertainty may make it very difficult to know what to expect for a child with only café-au-lait spots. In this respect, there is no way to predict the severity of NF1. Severely affected parents may have mildly affected children, and mildly affected parents may have severely affected children.
Despite the unpredictable nature of NF1, some common features of this genetic disorder include:
- Skin, bone, and eye abnormalities
- Nerve tumors
- Optic nerve and other brain tumors
- Learning and attention deficits
Skin, Bone, & Eye Abnormalities
Most individuals with NF1 have multiple café-au-lait macules and/or skinfold freckling. Individuals with NF1 are also more prone to developing bone and eye abnormalities.
Skin Abnormalities

Café-au-lait macules
Café-au-lait macules are flat, darkly pigmented spots or birthmarks on the skin, typically present at birth.
Skinfold freckling
These freckles are commonly seen in patients with NF1 in areas of the body not exposed to the sun, like the armpits and groin. They also may be found under the neck or under the breasts in women.
Bone Abnormalities
Children with NF1 are prone to the development of bone deformities involving the lower leg, forearm, and eye socket. Deformities of the lower leg and forearms can cause the bowing of these bones and lead to repeated fractures. Those bone problems involving the eye socket can affect how the eye sits in the socket. All of these bone deformities are typically noticed early in childhood and are treated promptly.
Eye Abnormalities
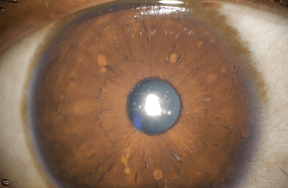
Some individuals with NF1 will have Lisch nodules, benign pigmented growths on the iris (the colored portion of the eye). They are usually found in both eyes but do not interfere with vision.
Nerve Tumors
Nerve tumors, known as neurofibromas, are benign or non-cancerous tumors that grow on nerves throughout the body. While they are seen in people without NF1, the presence of two or more of these tumors should raise suspicion of NF1. There are three major types of neurofibroma: cutaneous, spinal, and plexiform.
CUTANEOUS NEUROFIBROMAS
Also called discrete or dermal neurofibromas. these tumors grow from small nerves in the skin or just under the skin and appear as small bumps, typically beginning around the time of puberty. It is less common to see this type of neurofibroma in young children with NF1.
Individuals with NF1 commonly develop more cutaneous neurofibromas as they get older. In addition, women often notice that during pregnancy, they develop more neurofibromas or that existing neurofibromas grow larger. Cutaneous neurofibromas rarely cause medical problems but may itch or be tender when bumped. It is important to note that these tumors remain benign throughout life and do not become malignant cancers. Despite their benign nature, they may cause significant cosmetic problems and occasionally may require removal.
SPINAL NEUROFIBROMAS
Spinal neurofibromas are typically larger tumors that grow from nerves along the spinal column in adults with NF1. Despite the fact that spinal neurofibromas are close to the spinal cord, most people with spinal neurofibromas experience no medical problems as a result of their growth. Occasionally, adults with NF1 will experience back pain, numbness in an arm or leg, and minor weakness. People who develop these symptoms should consult a physician who is an expert in NF1.
PLEXIFORM NEUROFIBROMAS
Plexiform neurofibromas are larger, more extensive tumors that grow from nerves anywhere in the body. Unlike cutaneous neurofibromas, plexiform neurofibromas are often found in young children, sometimes even present around the time of birth. Plexiform neurofibromas may be located around the eye socket, face, arm, leg, back, chest, or abdomen.
Plexiform neurofibromas do not always stay benign throughout life, as cutaneous neurofibromas do. Uncommonly, a plexiform neurofibroma may change into a cancer, called a malignant peripheral nerve sheath tumor (MPNST). There are no reliable tests to screen for an MPNST.
Contact your NF specialist if you experience:
- Continued pain in your tumor (not associated with it being hit or bumped)
- Rapid tumor growth
- Hardening of the tumor
- Weakness or numbness in an arm or leg with a plexiform neurofibroma
These are signs that the plexiform neurofibroma may have changed into a cancer.
Optic Nerve & Other Brain Tumors
OPTIC NERVE GLIOMAS
Optic nerve gliomas are benign (non-cancerous) brain tumors that grow on the nerves that carry vision from the eyes to the brain (the optic nerves). Optic nerve gliomas are found in approximately one in five children with NF1.
These tumors commonly arise in young children and can affect their vision. For this reason, it is important that all children with NF1 have their vision checked yearly by an eye doctor (ophthalmologist) familiar with NF1. It is highly recommended that these yearly eye exams begin around one year of age and continue until children are at least ten years old.
Optic nerve gliomas are most commonly found using a specialized brain imaging test called magnetic resonance imaging, or MRI. A baseline MRI of the brain to look for optic nerve gliomas in young children with a normal eye exam is not necessary.
Most optic nerve gliomas in children with NF1 will not continue to grow and will not cause vision problems. Thus, knowing that a child has an optic nerve glioma is not an indication to begin treatment if there are no symptoms of tumor growth. Treatment should be reserved for children whose tumors are actively growing or resulting in worsening vision.
HYPOTHALAMUS & BRAINSTEM TUMOR
In addition to tumors that grow on the optic nerves, similar tumors in children with NF1 may grow in a region of the brain called the hypothalamus.
The hypothalamus is a part of the brain that is responsible for making hormones that trigger puberty. Brain tumors that grow in the hypothalamus (hypothalamic glioma) can cause young children to begin puberty. Parents should consult a physician who is an expert in NF1 if there is hair growth under the arms or in the pubic area in girls under seven, breast development in girls younger than seven, or enlargement of the penis and testicles in boys younger than eight.
Less commonly, brain tumors in children with NF1 may grow in other parts of the brain, including a region called the brainstem. Typically, brainstem gliomas in children with NF1 do not cause medical problems. Children with this type of brain tumor should be cared for by a physician who is an expert in NF1.
Treatment of brain tumors in children with NF1 typically involves drug therapy and not surgery or radiation. Children with NF1 who require treatment for their brain tumors should be managed by pediatric cancer specialists. Lastly, brain tumors in adults with NF1 are very rare but occur more commonly than they do in adults without NF1.
T2 HYPERINTENSITIES
Children with NF1 frequently will have T2 hyperintensities on magnetic resonance imaging (MRI) of the brain. They are commonly located in the optic nerve pathway, basal ganglia, cerebellum, and brainstem. These bright spots are not tumors and will not develop into brain tumors. T2 hyperintensities are most commonly seen in children and disappear in adulthood.
Learning & Attention Deficits
Fifty to sixty percent of children with NF1 will have some form of learning disability. NF1 patients typically have normal intelligence, but experience specific problems with reading, writing and the use of numbers.
Over 50% of children with NF1 also have issues with attention and executive function. Many of these children are successfully treated with medication and behavior therapy. In addition, problems with fine and gross motor skills are frequently encountered in children with NF1. Affected individuals are typically managed with physical and occupational therapy.
Learning disabilities in NF1

A learning disability can be thought of as a short circuit or problem (dysfunction) in one or several of channels in the brain. Dysfunction in any of these channels can make it harder for a child to perform up to their potential. These channels are important for getting information into the brain (input), processing that information, or communicating information (output). As a result, children with NF1 may have difficulty with reading, writing, math and memory, or have difficulty staying focused in the classroom.
Children with NF1 who experience difficulty getting information into the brain have a perceptual disability. Children with a perceptual disability can end up feeling confused, anxious and/or frustrated, and this can negatively impact their school performance and social interactions. These children may:
- Reverse letters
- Have problems with positioning objects in space
- Experience difficulties distinguishing subtle differences between similar sounds
- Misunderstand social cues and body language
Many children with NF1 may also have trouble processing information once it gets into the brain, and their brains may have difficulty making sense of the information they receive. These integration problems can include:
- Problems putting things in an order that makes sense
- Trouble figuring out the meaning of symbols and words
- Difficulty in organizing new information
Children with NF1, particularly boys, may additionally have difficulty communicating what they have learned, which is a problem with language and motor output. Children with this type of language problem can talk on and on, often with a great deal of intelligence and expression about a wide range of topics, and then freeze when asked a specific question.
Motor output problems can also be common in NF1, and these children are often regarded as clumsy or uncoordinated. Typically, they have difficulty with gym activities or with the fine motor coordination skills needed for writing.
For additional information about learning disabilities in NF1, check out:
Attention deficits in NF1

In addition to learning problems, a large number of children with NF1 have attention deficit disorder, with or without hyperactivity. Attention problems often co-exist with other learning disabilities. While attention deficit disorder may be obvious in some children with NF1, subtle, but still highly significant problems with attention may be uncovered in many children with NF1 only after formal testing. Those children with attention difficulties and/or hyperactivity benefit from behavioral modification or stimulant medication as well as special accommodations at school.
Supporting growth & learning in children with NF1
Despite these problems, most children have relatively normal intelligence. Importantly, children with learning disabilities are not stupid or lazy. They have significant problems with the way they learn and perceive the world, and require alternative strategies to support their growth and learning.
Their problems should be formally evaluated by a professional either privately or in the school district to develop an appropriate individualized education plan (IEP). Those children who do not qualify for an IEP may receive services through a 504 plan. Children with NF1, who receive these intensive services, will have the greatest chance of living up to their potential.